Modern implant dentistry has transitioned from a predominantly surgically driven discipline to a prosthetically oriented, outcome-focused workflow. Central to this evolution is the concept of prosthetically driven (prosthodontically driven) implant placement, which is now widely regarded as a fundamental principle of contemporary implant therapy, particularly in esthetic and complex rehabilitation cases [1–3].
Concept and Definition
Prosthetically driven implant placement refers to a planning philosophy in which the final prosthetic restoration dictates implant position, angulation, depth, and distribution, rather than placing implants based solely on available bone [1,4]. In this approach, the clinician first defines the ideal position of the definitive restoration in terms of esthetics, occlusion, phonetics, and function. Implant placement is then planned three-dimensionally to optimally support that restoration.
Historically, implants were frequently placed wherever bone volume permitted, with prosthetic compromises made afterward. Such workflows often resulted in unfavorable emergence profiles, non-ideal screw-access locations, biomechanical overload, and compromised esthetic outcomes [2,5]. Prosthetically driven planning reverses this logic, placing restorative goals at the center of treatment planning.
Rationale for a Prosthetically Driven Approach
The rationale for prosthetically driven implant placement is supported by biomechanical and biological principles. Implant position and angulation directly affect force distribution, stress concentration, and long-term marginal bone stability [6]. From an esthetic perspective, especially in the anterior region, three-dimensional implant positioning is critical for achieving harmonious soft-tissue contours, papilla preservation, and natural crown morphology [7].
Importantly, prosthetic-first planning allows clinicians to identify cases where hard- or soft-tissue augmentation is necessary prior to implant placement. Rather than compromising the restoration, the biological environment is modified to support the ideal prosthetic outcome [3,8].
Digital Workflow and Guided Implant Surgery
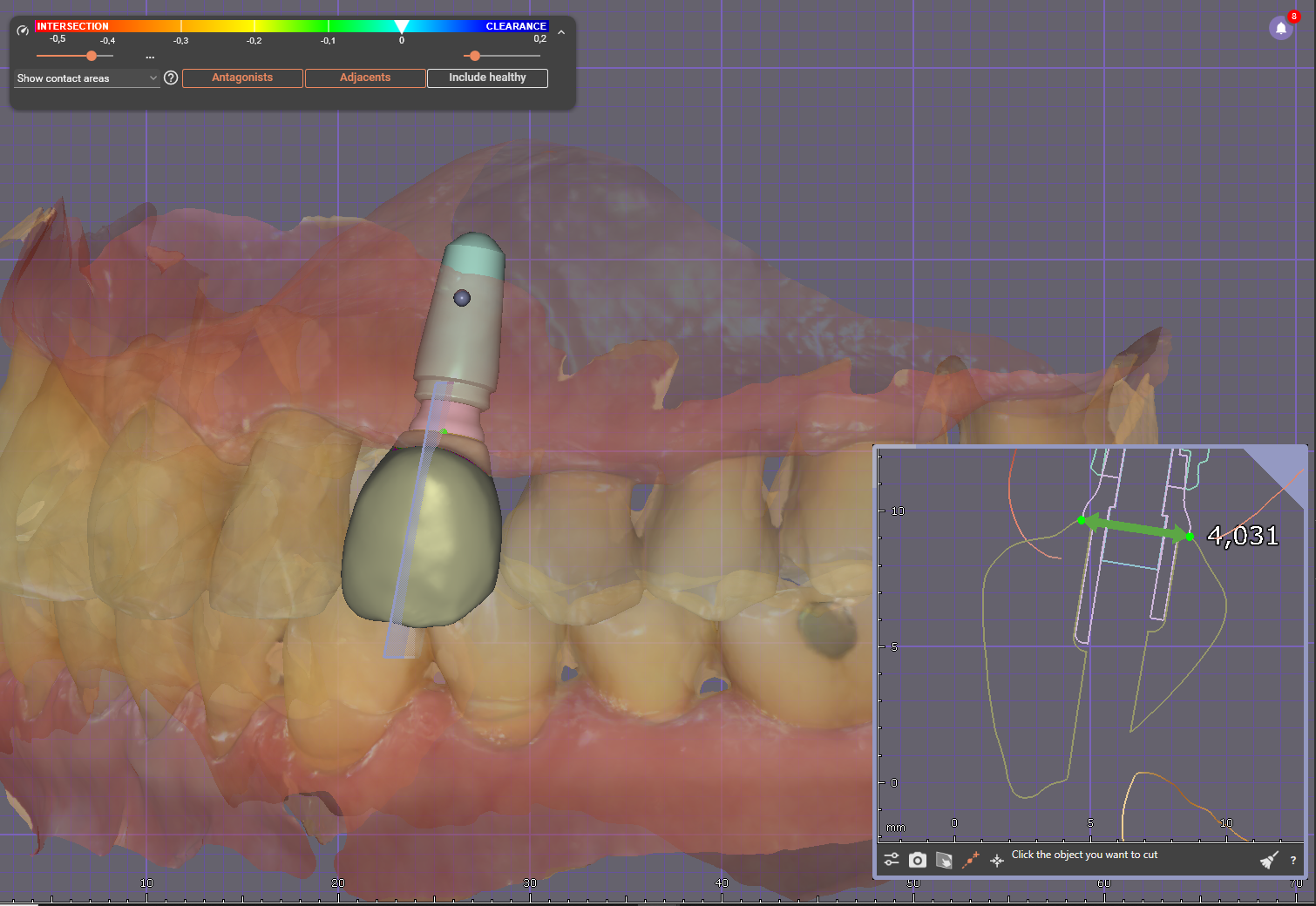
The integration of cone-beam computed tomography (CBCT), intraoral scanning, and CAD/CAM technologieshas made prosthetically driven implant placement more accurate and reproducible. By superimposing CBCT data with a digital wax-up, clinicians can visualize the planned restoration relative to the alveolar bone and critical anatomical structures [9,10].
This virtual plan can be transferred to the surgical field using static surgical guides or dynamic navigation systems. These technologies aim to replicate the planned implant position with minimal deviation, reducing operator-dependent variability and improving alignment with prosthetic objectives [11].
Scientific Evidence Supporting the Concept
Although prosthetically driven implant placement is a planning philosophy rather than a single intervention, its scientific support is robust and multifactorial. Systematic reviews evaluating guided implant surgery consistently demonstrate that computer-guided approaches achieve greater positional accuracy compared with freehand placement [12–14].
Meta-analyses report mean coronal and apical deviations of approximately 1–1.5 mm and angular deviations around 3–4°, values that are generally superior to those observed with conventional techniques [12,13]. These deviations are clinically significant, as small angular errors may result in major prosthetic complications, particularly in screw-retained restorations.
Randomized and prospective clinical studies further support these findings. Trials comparing fully guided, partially guided, and freehand implant placement show that fully guided protocols achieve significantly higher trueness relative to the virtual prosthetic plan [15,16]. This is especially relevant in full-arch rehabilitations, where cumulative positional errors can compromise prosthetic fit and passivity.
While implant survival rates between guided and non-guided placement are generally comparable, guided and prosthetically planned approaches demonstrate advantages in prosthetic accuracy, emergence profile control, and reduction of restorative complications [14,17]. These benefits are particularly evident in esthetically demanding zones and in immediate or early loading protocols.
Furthermore, studies evaluating the influence of operator experience suggest that guided workflows reduce inter-operator variability, supporting the concept that prosthetically driven planning contributes to standardization and predictability in implant therapy [18].
Clinical and Educational Consensus
Beyond individual studies, prosthetically driven implant placement is strongly endorsed in contemporary textbooks, consensus statements, and professional guidelines. Authors consistently emphasize that implant placement should be restoration-driven and that anatomical limitations should be addressed through site development rather than prosthetic compromise [1,3,6].
This consensus reflects a broader shift toward interdisciplinary treatment planning, involving surgeons, prosthodontists, and dental technicians from the earliest stages of care.
Conclusion
Prosthetically driven implant placement represents a cornerstone of modern implant dentistry. By prioritizing the final restorative outcome and employing digital planning and guided execution, clinicians can achieve superior esthetic, functional, and biomechanical results. The scientific literature—including systematic reviews, randomized trials, and clinical studies—supports the accuracy, predictability, and restorative advantages of this approach.
In contemporary practice, success in implant dentistry is no longer defined by implant survival alone, but by the quality, longevity, and predictability of the final prosthesis. Prosthetically driven planning is therefore essential for achieving optimal outcomes in modern implant rehabilitation.
References
- Garber DA. The esthetic dental implant: letting restoration be the guide. J Am Dent Assoc. 1995;126(3):319–25.
- Buser D, Martin W, Belser UC. Optimizing esthetics for implant restorations in the anterior maxilla. Int J Oral Maxillofac Implants. 2004;19 Suppl:43–61.
- Misch CE. Dental Implant Prosthetics. 2nd ed. St. Louis: Mosby; 2015.
- Katsoulis J, Pazera P, Mericske-Stern R. Prosthetically driven, computer-guided implant planning for the edentulous maxilla: a model study. Clin Implant Dent Relat Res. 2009;11(3):238–45.
- Belser UC, Bernard JP, Buser D. Implant-supported restorations in the anterior region: prosthetic considerations. Pract Periodontics Aesthet Dent. 1996;8(9):875–83.
- Rangert B, Jemt T, Jörneus L. Forces and moments on Branemark implants. Int J Oral Maxillofac Implants. 1989;4(3):241–7.
- Kan JY, Rungcharassaeng K. Facial gingival tissue stability following immediate placement and provisionalization of maxillary anterior single implants. Int J Oral Maxillofac Implants. 2003;18(1):31–9.
- Buser D, Chen ST, Weber HP, Belser UC. Early implant placement following single-tooth extraction in the esthetic zone. Int J Oral Maxillofac Implants. 2008;23(5):841–51.
- Tahmaseb A, Wismeijer D, Coucke W, Derksen W. Computer technology applications in surgical implant dentistry: a systematic review. Int J Oral Maxillofac Implants. 2014;29 Suppl:25–42.
- Vercruyssen M, Laleman I, Jacobs R, Quirynen M. Computer-supported implant planning and guided surgery: a narrative review. Clin Oral Implants Res. 2015;26 Suppl 11:69–76.
- Block MS, Emery RW. Static or dynamic navigation for implant placement—choosing the method of guidance. J Oral Maxillofac Surg. 2016;74(2):269–77.
- Van Assche N, et al. Accuracy of guided implant surgery: a systematic review and meta-analysis. Clin Oral Implants Res. 2012;23 Suppl 6:73–86.
- D’haese J, et al. Accuracy of computer-aided implant placement: a systematic review. Clin Oral Implants Res. 2012;23 Suppl 6:112–23.
- Tahmaseb A, et al. Guided implant surgery: a systematic review and meta-analysis. Int J Oral Maxillofac Implants. 2018;33(2):331–48.
- Vercruyssen M, et al. Comparison of accuracy between guided and freehand implant placement: a randomized clinical trial. Clin Oral Implants Res. 2014;25(5):616–22.
- Schnutenhaus S, et al. Accuracy of fully guided implant placement in edentulous jaws. BMC Oral Health. 2025;25:73.
- Nulty A. Prosthetically designed guided implant placement and factors influencing implant success. Br Dent J. 2024;236(3):153–60.
- Schneider D, et al. Impact of surgeon experience on the accuracy of guided implant surgery. J Prosthet Dent. 2024;131(2):211–8.